Tachycardia ACLS Algorithm
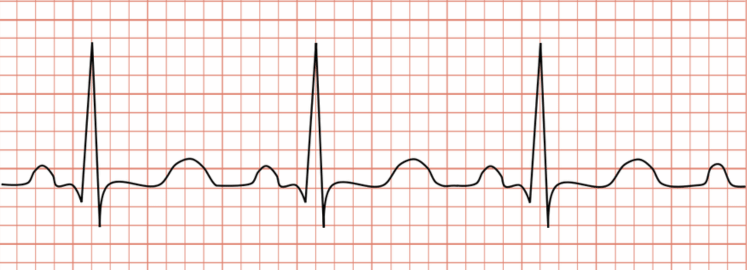
The normal heart beats at the rate of 60 - 100 times per minute while at rest. When the heartbeat rate consistently exceeds 100 beats per minute, usually rates above 150 bpm, the condition is considered Tachycardia. It leads to low cardiac output and as a result, it reduces oxygen saturation level and perfusion in the patient’s body. The ACLS Tachycardia Algorithm is a part of the Advance Cardiac Life Support (ACLS) algorithm used in emergency medicine to manage patients with fast heartbeat.
A variety of factors, both physiological and pathological, can cause tachycardia. Few common causes include fever, dehydration, shock, stress, pain, anxiety, hypoxemia (low blood oxygen), stimulant use, and certain medications. In addition to these, underlying heart conditions, thyroid imbalances, or electrolyte disturbances can also trigger fast heart rhythms or elevated heart rate. Here are the steps of Tachycardia With a Pulse Algorithm:
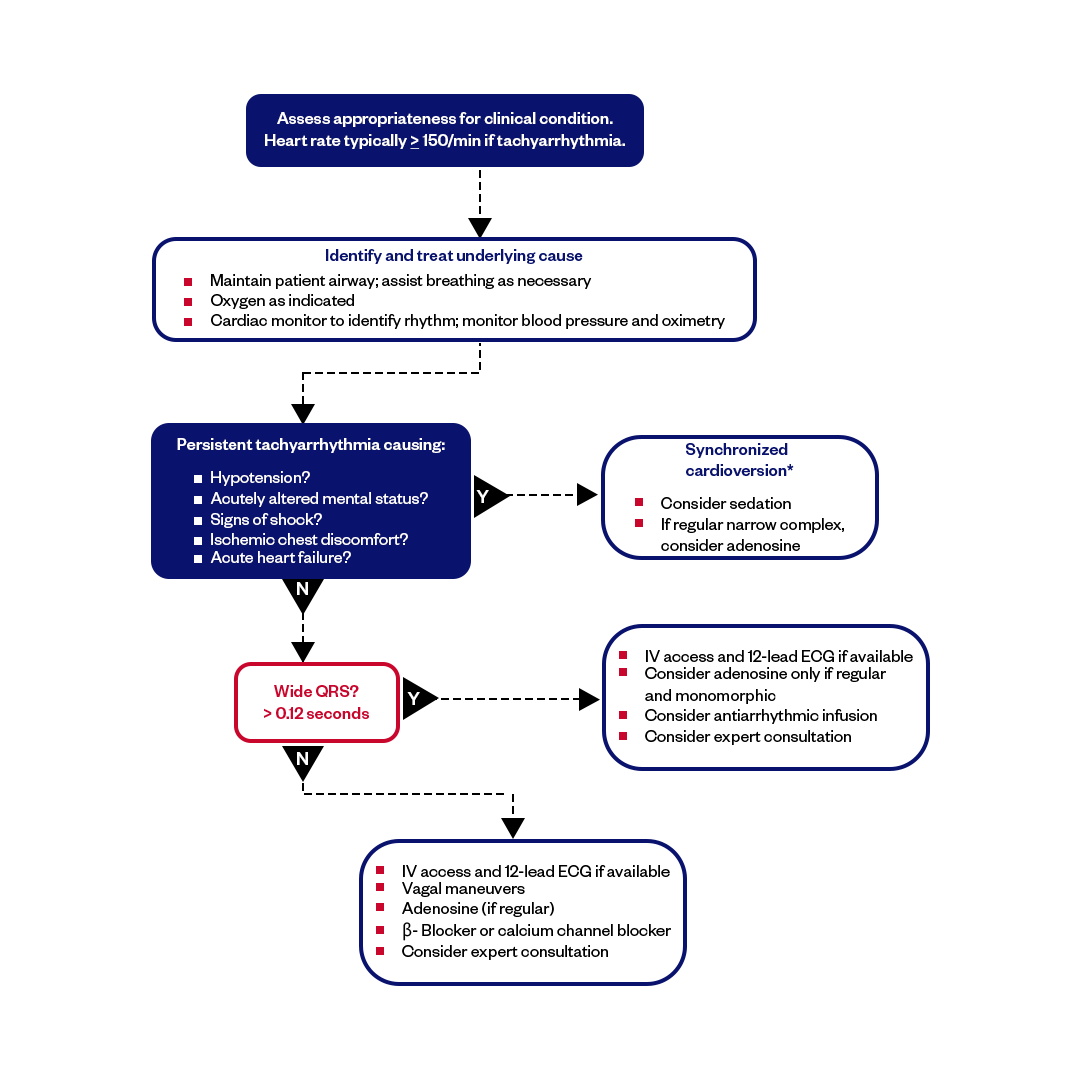
Image: Tachycardia With a Pulse Algorithm
Signs and Symptoms of Tachycardia
Heart pounding, a sensation of racing, chest pain, fainting, altered mental status, and a rapid pulse rate are common symptoms of tachycardia. It's rare to have these symptoms when the heart rate ranges between 100 to 150 beats per minute (bpm) but if it goes higher, then the symptoms are likely to occur.
Here are the common signs and symptoms of Tachycardia:
1) Heart palpitations
2) Chest discomfort or pain
3) Dizziness or unsteadiness
4) Fatigue
5) Shortness of breath
6) Fainting
7) Rapid pulse
8) Hypotension (Low blood pressure)
9) Anxiety or a sense of unease
ACLS Algorithm for Tachycardia treatment
The ACLS algorithm for tachycardia helps healthcare providers make rapid and accurate medical intervention based the specific type and underlying causes of the condition, severity of the symptoms, patient's stability, electrocardiogram (ECG) findings, and response to ongoing treatment. Here are the step-by-step approach of the ventricular tachycardia ACLS algorithm that a rescuer should follow:
- Assess the Patient
- Obtain a 12-lead Electrocardiogram (ECG)
- Determine the Tachycardia Type
- Assess Vital Signs
- Consider Underlying Causes
- Vagal Maneuvers
- Administer Medications
- Synchronized Cardioversion
- Monitor Continuously
The Treatments in ACLS Tachycardia Algorithm for a patient experiencing different tachycardia are as follows:
Supraventricular Tachycardias (SVT):
Vagal Maneuvers: Attempt vagal maneuvers like the Valsalva maneuver, carotid sinus massage, or cold stimulus to the face.
Adenosine: Administer adenosine as a rapid intravenous (IV) bolus. It's often the first-line medication for SVT.
Beta-Blockers or Calcium Channel Blockers: In stable cases, oral or IV beta-blockers (e.g., metoprolol) or calcium channel blockers (e.g., diltiazem) may be used.
Atrial Fibrillation (AF) and Atrial Flutter:
Rate Control: Use medications such as beta-blockers, calcium channel blockers, or digoxin to control increased heart rate.
Rhythm Control: Administer anti-arrhythmic medications like amiodarone or flecainide to restore and maintain normal sinus rhythm.
Anticoagulation: Consider anticoagulant therapy to prevent thromboembolic events in patients with Atrial fibrillation at risk.
Ventricular Tachycardia (VT):
Stable VT: Administer anti-arrhythmic drugs like amiodarone or lidocaine.
Unstable VT: Perform synchronized cardioversion using appropriate energy levels.
Consider Magnesium: Consider IV magnesium sulfate in cases of torsades de pointes or suspected magnesium deficiency.
Wide-Complex Tachycardia of Unknown Origin:
Stable Wide-Complex Tachycardia: For stable WCT with a wide QRS complex, administer IV amiodarone.
Unstable Wide-Complex Tachycardia: Perform immediate synchronized cardioversion.
Sinus Tachycardia:
Identify and Treat Underlying Cause: Address and manage the underlying condition causing sinus tachycardia, such as pain, fever, or anxiety.
Beta-Blockers: Consider beta-blockers if appropriate for symptom control.
Atrioventricular Nodal Reentrant Tachycardia (AVNRT) and Atrioventricular Reentrant Tachycardia (AVRT):
Vagal Maneuvers: Attempt vagal maneuvers.
Adenosine: Administer adenosine as a rapid IV bolus.
If unsuccessful: Consider other anti-arrhythmic medications or catheter ablation for recurrent episodes.
Wolff-Parkinson-White (WPW) Syndrome:
Procainamide or Amiodarone: Administer procainamide or amiodarone for acute management.
Definitive Treatment: Catheter ablation is often recommended to eliminate the accessory pathway responsible for WPW syndrome.
Note: Specific treatment protocols may vary based on the patient's clinical condition, and healthcare providers must follow guidelines for current treatment and individualized patient care plans. Treatment choice depends on the type of tachycardia, the patient's clinical presentation, and any underlying medical conditions.
Medication Doses and Details
Adenosine IV dose:
- Adenosine is administered intravenously in two doses: Initial dose: 6mg rapid IV followed by NS flush
- 2nd dose: 12mg if needed
Procainamide IV dose:
20-50mg/min IV
Synchronized Cardioversion rules:
- QRS narrow and regular: 50-100 J
- QRS narrow and irregular: 120-200 J
- QRS wide and regular: 100 Joules
- QRS wide and irregular: Immediately defibrillate (not synchronized)
Amiodarone IV dose:
150mg over 10 min
Sotalol IV dose:
100mg over 5 minute
Final Thoughts
The treatment for Tachycardia follows the ACLS Tachycardia Algorithm, which is a systematic approach based on ACLS protocols. It serves as a critical guide for healthcare professionals to assess and manage the risks associated with rapid heartbeat conditions and ensures better patient outcomes.
Fast and Convenient
Take ACLS Classes
*Nationally Accepted
ACLS
CERTIFICATION
AHA ACLS course
State-of-the-Art Facilities
Unlimited Exam Retakes
$260
ACLS
ONLINE CERTIFICATION
AHA ACLS Online Course
100% online training
Unlimited Exam Retakes
$280
FAQs of ACLS Tachycardia Algorithm
What are the symptoms of tachycardia?
It could be a sign of tachycardia if you’re experiencing symptoms like chest pain, a rapid or pounding heartbeat, dizziness, shortness of breath, or even fainting. Some victims also feel really anxious or have a sense that something just isn’t right. In more serious cases, it can even lead to cardiac arrest. If you notice any of these symptoms, it’s important to seek medical help right away.
What is the most common tachycardia?
Atrioventricular Nodal Reentrant Tachycardia (AVNRT) is the most common form of supraventricular tachycardia, accounting for over 60% of cases. It occurs due to an abnormal electrical circuit within or near the atrioventricular (AV) node, causing the heart to beat rapidly.
What do you do for tachycardia?
The best treatment for tachycardia depends on the cause and type. Initial steps include vagal maneuvers like coughing or using an ice pack. If those don’t work, doctors may use medications, electrical cardioversion, or catheter ablation for long-term management.
How long is too long for tachycardia?
If tachycardia lasts longer than 30 minutes, especially with symptoms like shortness of breath and chest pain, it may indicate a serious condition such as Supraventricular Tachycardia (SVT). This requires immediate medical attention. Call 911 or go to the nearest emergency room if symptoms persist.
How long can your heart stay in tachycardia?
Tachycardia can last anywhere from seconds to minutes, or even hours. In some cases, it may occur repeatedly throughout the day. During an episode, the heart rate can reach up to 250 beats per minute (bpm), depending on the type and severity of the condition.
What is the first drug of choice in a tachycardia according ACLS guidelines?
According to ACLS guidelines, the first drug of choice in stable tachycardia with a narrow QRS complex is adenosine, given as a rapid IV push of 6 mg followed by a normal saline flush. If the rhythm is regular and monomorphic, adenosine may also be considered for unstable patients before synchronized cardioversion. Expert consultation should be strongly considered for stable wide QRS complex tachycardia, and antiarrhythmic infusions such as procainamide, amiodarone, or sotalol IV may be used.
What are the non-drug therapies for tachycardia?
Procedures like vagal maneuvers, carotid massage, or Valsalva maneuvers are non-drug therapies used to manage certain types of tachycardia.

Owner Jeff Haughy has been providing high-quality care in the EMS industry since 1995 and started his Fire Service career with the Alameda Fire Department in 1991 as a Fire Explorer.